

Welcome to Amanda's NICU Education


Hi! My name is Amanda. I'm a NICU nurse, Clinical Nurse Specialist, NICU Educator... basically your NICU BFF. If you want to talk NICU, I'm here for you! I love everything about NICU nursing and I'm eager to learn and share my knowledge with all my NICU friends.
I have been a NICU nurse since 2009 I am currently a Clinical Nurse Specialist in a Level IV NICU in Los Angeles.
I am passionate about educating the next generation of NICU nurses. I share my knowledge through platforms such as Instagram and Facebook and am excited to have you here on my website!
Click on the button below to sign up for my newsletter filled with NICU education and tips for all experience levels.

Not very many people love taking tests but as a self-acclaimed "forever student" who has taken (and passed) five different certification exams I am no longer afraid of tests! "Way to brag", you might be thinking but I want to help YOU pass your certification exam too!
Introducing Amanda's RNC-NIC Success digital course - your ultimate study companion!
Gain unlimited, on-demand access for life, ensuring you're primed to ace your certification exam.
I'm here to help you succeed and I can't wait for you to share with me that you PASSED the RNC-NIC EXAM!!!








Respiratory Distress (part 2)
"Neonates are at particular risk for pneumonia due to their immature innate and adaptive immunity..."
Respiratory Disorders in the NICU: Part 2
As we reviewed earlier this month one of the most common reasons babies end up in the NICU is due to respiratory distress. Let's get back to basics and review some of the other respiratory disorders that we see in the NICU.
In part 2 of this respiratory disorder series, let's review Neonatal Pneumonia and Meconium Aspiration Syndrome.
Neonatal Pneumonia
Pneumonia is an infection of the lungs that can be caused by bacteria, viruses, or fungi. Neonates are at particular risk for pneumonia due to their immature innate and adaptive immunity. Additional risk factors for pneumonia include maternal colonization with pathogens, prolonged rupture of membranes, prematurity, prolonged hospitalization, mechanical ventilation causing injury to the respiratory epithelium, and gastroesophageal reflux.
Congenital pneumonia can occur after intrauterine infection, asphyxia, or a combination of both. When there is maternal colonization of pathogens, those pathogens can ascend into the birth canal. When there is rupture of membranes those pathogens can contaminate the amniotic fluid which is aspirated by the fetus. The most common pathogens that cause congenital pneumonia include Group B Streptococci and E. Coli. (Know that for the certification exam if you're prepping).
After birth neonates can acquire pneumonia from passage of pathogens from equipment and caregivers. Neonates who require mechanical ventilation are at risk for Ventilator Associated Pneumonia (VAP) or a Ventilator Associated Event (VAE). VAP and VAE are nosocomial complications of mechanical ventilation. The most common pathogens include coagulase-negative Staphylococci , Staphylococcus aureus , Gram-negative rods (e.g., E. Coli, Pseudomonas ), and Candida.
Prevention is key when it comes to neonatal pneumonia. In the prenatal and intrapartum period, mothers are screened for GBS colonization and other infections. If bacterial infections are present (or colonization of GBS is unknown) they are managed with antibiotics.
Similarly, when babies are in the NICU, prevention of infection is paramount. Meticulous hand hygiene practices, equipment disinfection, early extubation and the use of noninvasive mechanical ventilation are all strategies to prevent VAP and VAE. Many NICUs utilize a "VAP Bundle" to prevent pneumonia in their patients. Important aspects of the bundle include hand hygiene, oral care, head of bed elevation, repositioning, guidance around suctioning, and ventilator circuit changes. Does your NICU have a VAP bundle? What is in it?
Clinical manifestations of a baby with pneumonia include signs of respiratory distress that can be nonspecific and difficult to distinguish from other respiratory disorders at birth. Additional signs include, temperature instability, apnea, tachycardia or bradycardia, increased and potentially discolored respiratory secretions, desaturations, and distress requiring increased ventilator settings.
Serial X-Rays may be helpful as the appearance on X-Ray can vary depending on the duration of infection. We may see pleural effusion, reticulo-nodular densities, or patchy and asymmetric infiltrates with areas of hyperaeration.
Treatment of Neonatal Pneumonia is supportive and includes antibiotics if the causative organisms was bacterial, antivirals for viral pneumonia, and anti-fungals for fungal pneumonia.
Meconium Aspiration
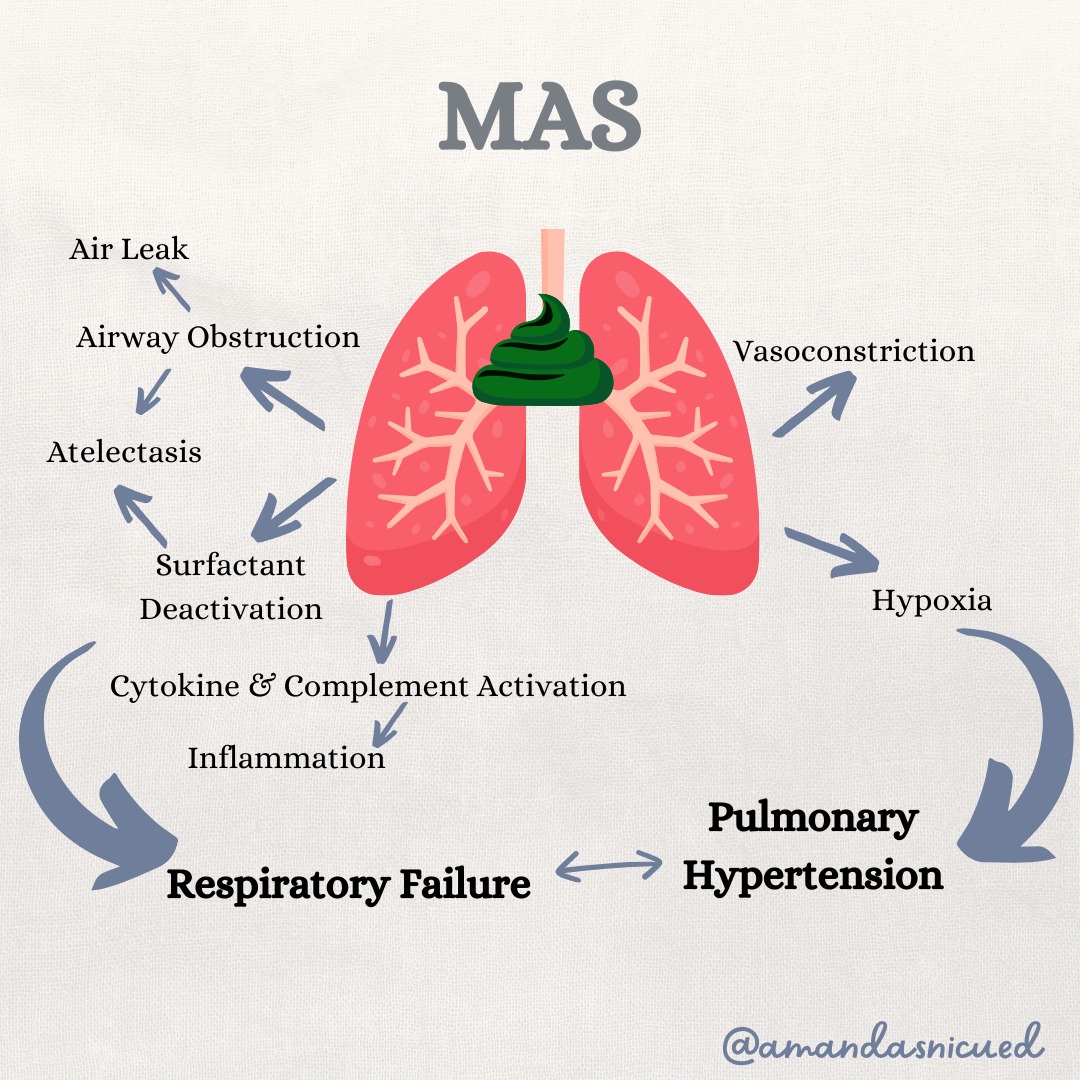
Meconium Aspiration Syndrome (MAS) occurs when a newborn born through meconium stained amniotic fluid (MSAF) has respiratory distress that cannot be explained by any other etiology. Meconium contains proinflammatory components such as bile acids and enzymes, as well as vernix, hair, epithelial cells, mucus, and blood. The pathophysiology of MAS is not completely understood. When the fetus experiences stress and hypoxic events in utero the fetus begins gasping and aspiration of amniotic fluid can occur. The hypoxic event also stimulates peristalsis and anal relaxation causing the fetus to pass meconium in utero. Aspiration of meconium causes multifactoral disease including partial or complete obstruction of the airways, inflammation, cytokine activation, surfactant deactivation, apoptosis of epithelial cells, and increased pulmonary vascular resistance.
When the meconium is aspirated it causes partial or complete obstruction which results in collapse of the alveoli (atelectasis). Partial obstruction can result in air trapping, or a "ball valve" effect. Basically, air can get in but it can't get out which subsequently can cause an air leak.
The proinflammatory components of meconium causes inflammation and a release of cytokines to the alveoli manifesting as a chemical pneumonitis. The inflammation and plasma proteins leaking into the alveoli can cause destruction to the type II alveolar cells resulting in decreased release of surfactant.
Fetal and neonatal hypoxemia can induce pulmonary vasoconstriction, preventing the normal decrease in pulmonary vascular resistance. Further infants born with meconium aspiration syndrome have acidosis which contributes to pulmonary hypertension. The increased pulmonary vascular resistance may lead to right to left shunting and further hypoxemia.
What might we see when caring for a baby with MAS? The clinical presentation can vary from mild to severe. Typically these newborns are born term or post-term. Many babies delivered through MSAF do not have distress at birth. However some babies will present with poor respiratory effort, decreased tone, cyanosis and they may also present with perinatal asphyxia. Depending on the duration of exposure to meconium, the skin, nails, and vernix may be stained a yellow/green color.
The chest X-Ray will typically show hyperinflations and flattened diaphragms with coarse, irregular patchy infiltrates. Air leaks, such as pneumothorax or pneumomediastinum, may be present. Additionally, pulmonary hypertension may be seen on echocardiogram.
The management of newborns delivered through MSAF has evolved over the years. Prevention of MAS is ideal through identifications of high risk pregnancies and appropriate monitoring during labor. Interestingly, amnioinfusion (instilling isotonic fluid into the amniotic cavity) was not found to improve outcomes in settings with standard peripartum and expert neonatal care.
In the delivery room, a skilled resuscitation team must be present for infants with MSAF and the management will vary depending on whether the baby is vigorous or not. Routine care is performed for the vigorous infant, with spontaneous breathing, and a HR >100. The nonvigrous infant who is depressed or as inadequate tone or respirations should be resuscitated. Secretions can be cleared from the nose and mouth with a bulb syringe. If the newborns HR is <100 and/or the newborn is not effectively breathing, positive pressure ventilation (PPV) is indicated. Observe for signs of effective ventilation (increasing heart rate and chest rise) and take corrective steps using MR SOPA and needed. If the infant is not improving, or there is no chest rise, suspect an airway obstruction. Attempt to clear the airway with a suction catheter inserted into the endotracheal tube or utilize a meconium aspirator. A meconium aspirator attaches to the suction source then directly to the endotracheal tube. To suction, occlude the control port on the aspirator and gently withdraw the tube over 3-5 seconds. Be prepared to resume PPV with a face mask.
In the NICU, management of the newborn with MAS is supportive. These babies require minimal handling to prevent agitation and may need sedation. The severity of MAS will determine the level of respiratory support the baby needs. Supplemental oxygen is provided with the goal of preventing hypoxia and trying to maintain an oxygen tension range around 80-90 mmHg. Those with severe MAS may require high frequency ventilation. If pulmonary hypertension is present, inhaled nitric oxide has been shown to be beneficial. Surfactant replacement may also be given to decrease the severity of respiratory illness. Data has shown providing surfactant has decreased the duration of mechanical ventilation, hospital length of stay, and the need for ECMO.
When caring for these babies, maintaining an adequate blood pressure and perfusion is necessary. Infants may need volume expansion, vasopressor support, or packed red blood cell transfusion to maintain a hematocrit >40%. Perfusion and oxygen carrying capacity is essential to optimize oxygen delivery to the tissue. Infants who have MAS that is refractory to all the support mentioned can be placed on Extracorporeal life support (ECLS also known as ECMO).
Infants with severe MAS may have neurologic sequelae and even death despite maximal support. The nurse is an essential member of the NICU team to care for the baby and their family during their difficult NICU stay.
Neonatal Resuscitation
How strong do you feel in your neonatal resuscitation skills? Did you know the AAP and NRP have a bunch of videos demonstrating many of the skills that are essential to an effective resuscitation. Whether you are prepping for the certification exam, or just want to brush up on your skills, take a look at the videos in the link below.
Click Here for Videos from the AAP & NRP

I hope you are enjoying this review of neonatal respiratory disorders during the month of January. In our next newsletter let's cover PPHN and air leaks.
I love hearing from you, reach out to me with any questions you have or ideas for future blogs! 😊
Wishing you all the best!
Amanda xoxo
Missed my other newsletters? Click here to read them!
Let's Study Together! Join my Certification Course
References:
Crowley, M. Neonatal Respiratory Disorders in Fanaroff, et al., Klaus & Fanaroff's Care of the High-Risk Neonate, Elsevier-Saunders, 2020
Wilson, J., & Fitzgerald, J. The Respiratory System in Jnah & Trembath's Fetal & Neonatal Physiology for the Advanced Practice Nurse. Springer 2018
Center for Disease Control & Prevention (2024). Pediatric Ventilator Associated Event. Retrieved from https://www.cdc.gov/nhsn/pdfs/pscmanual/pedvae-current-508.pdf on January 6, 2024
The American College of Obstetrics & Gynecology. (2019). Prevention of Group B Streptococcal Early Onset Sepsis in Neonates. Retrieved from https://www.acog.org/clinical/clinical-guidance/committee-opinion/articles/2020/02/prevention-of-group-b-streptococcal-early-onset-disease-in-newborns on January 6, 2024
Fraser, D. (2021) Respiratory Distress in Verklan, et al.'s, Core Curriculum for Neonatal Intensive Care Nursing, Elsevier.
Textbook of Neonatal Resuscitation, 8th Ed. American Academy of Pediatrics and American Heart Association; 2021.
Gomella, Neonatology, 8th ed., Lange, 2020.


December 2023 Certification Review Webinar
NICU Certification Review


Ready to kickstart your journey to becoming a certified NICU nurse?
Look no further!
Grab my FREE E-Book packed with essential study and test-taking strategies for the RNC-NIC.
In the E-Book I give you the resources you need including the link to access the candidate guide, several types of books to study from, some of my favorite strategies, an outline of the content you should review, and a blank calendar for you to make your study plan!
Frequently Asked Questions About the RNC-NIC exam

What is the RNC-NIC?
The RNC-NIC is a competency-based exam that tests the specialty knowledge of nurses in the United States & Canada who care for critically ill newborns and their families.
The RNC-NICU is a nationally recognized certification that recognizes the registered nurse for their specialty knowledge and skill.

Who can take the RNC-NIC exam?
Nurses can take this exam after a minimum of two years experience in the NICU caring for critically ill newborns and their families.

Which books should I use?
I'm glad you asked! There are many excellent books to help you prepare for the RNC-NIC, I gathered ande describe each of them for you in my FREE e-book.
Is there a course to help me study?
Yes! Many hospitals host their own certification course and there are a few online courses. See my RNC-NIC test taking tips E Book for more information
What happens if I don't pass the exam?
If you don't pass the exam on your first try you can try again after 90 days. You will have to reapply after 90 days and pay a retest fee. There is no limit to the number of times you can take the exam (however a candidate can only sit for the exam twice per year).

Can I make more money if I take the RNC-NIC exam and get certified?
Yes! Many hospitals provide a raise or a bonus for nurses with specialty certifications. Hospitals also typically hire at a higher base salary when nurses have a certification.

Find me @amandasnicued on these channels or Email me
hey nurses don't miss out
© Copyright 2024. AmandasNICUEd. All rights reserved. | Terms & Conditions | Privacy Policy Contact: [email protected]